no. What Is The Code Next To The Main Term Called? Jette N, Quan H, Hemmelgarn B, et al. This is a list of codes which have been placed in numerical order. Hospital-based medical records are abstracted to create International Classification of Disease (ICD) coded discharge health data in many countries. The fact that the stroke occurred following hospitalization would be missed if it were coded as the main condition. There are two definitions that have been used for the main condition in ICD-coded health data: a resource use definition and a reason for admission definition.
official website and that any information you provide is encrypted The coder should revert to the default rule that allows the selection of the first condition recorded by the responsible clinician in circumstances where there is more than one main condition treated and no information is available to determine which of the conditions is the most severe or life threatening, or which one is responsible for the greatest use of resources. These codes are applied to different kinds of emerging technologies. A normal term is any time when this lease lasts until the final day of the fifteenth Rent Year (as long as the conditions specified in this Lease apply). Patients in the same CMG are assumed to be relatively homogeneous.
This recommendation of dual coding of reason for admission and resource use key conditions was presented to WHO-FIC Network member countries at the Network's annual meeting in Brasilia, Brazil in October 2012. This recommendation is made with recognition that determining the main condition can be complex. The WHO Topic Advisory Group for Quality and Safety membership includes: William Ghali (co-chair), Harold Pincus (co-chair), Marilyn Allen, Susan Brien, Bernard Burnand, Cyrille Colin, Saskia Droesler, Alan Forster, Yana Gurevich, James Harrison, Lori Moskal, William Munier, Donna Pickett, Hude Quan, Patrick Romano, Brigitta Spaeth-Rublee, Danielle Southern and Vijaya Sundararajan. If no diagnosis was made, the main symptom, abnormal finding or problem should be selected as the main condition. about navigating our updated article layout. operating room time, investigative technology, etc.) They are added to the end of a code with a hyphen. Drs Hude Quan and William Ghali are funded by Alberta Innovates Health Solutions (AI-HS). This stands for the Current Procedural Terminology that has been established by the American Medical Association. Describe the set of instructions you follow to solve a problem using an algorithm. It is also called the International Classification of Diseases, the 10th Revision, Clinical Modification code, for diagnosis codes of diseases like the ICD-10-CM.An individuals disease or medical condition can be described by these codes. Charlson ME, Pompei P, Ales KL, et al. Some countries employ a reason for admission coding rule, while others employ a resource use coding rule. bypass coronary artery graft cabg surgery illustration Key components of the revision process are Topic Advisory Groups (TAGs), which serve as the planning and coordinating advisory bodies for specific issues that are key topics in the revision process. The QS-TAG recommends that the term main condition should be discarded in the context of ICD-coded hospital data because its definition is inconsistent and confusing. If there is more than one such condition, the one held most responsible for the greatest use of resources should be selected. In Australia, the definition for main condition is: The diagnosis established after study to be chiefly responsible for occasioning an episode of admitted patient care, an episode of residential care or an attendance at the health care establishment, as represented by a code [8]. Note that the current WHO definition does not stipulate whether the main condition must be present at the beginning of the hospital admission. knock knees bow body knocked legs correct legged exercises army indian knee touching normal treatment correction exercise joint help In our opening clinical scenario, AMI as the condition leading to admission and stroke as the condition leading to the most resource use could both be coded and understood simultaneously for their relevance to the patient's hospital course.
{kind=link}
{kind=link}
It is a form that makes patients aware of that fact. Acute myocardial infarction in Alberta: temporal changes in outcomes, 1994 to 1999. Outcomes after acute myocardial infarction in South Asian, Chinese, and white patients. These codes are used to identify conditions that are not considered an injury or illness. Clearly, understanding which of these definitions of main condition is being used is important to data users, because the main condition coding rule can influence case selection and inferences made from coded health data. Ideally, all countries undertaking ICD coding of hospital episodes would code both the reason for admission and resource use as key conditions in their ICD-coded health data. This is a four-digit code, which serves the purpose of describing the code in greater detail. The development, evolution, and modifications of ICD-10: challenges to the international comparability of morbidity data. A few countries have recently transitioned from one of these approaches to the other.
In the USA, the term principal diagnosis is used and is defined as that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care [7]. For example, ALS is commonly called Lou Gehrigs disease. Such differences in the CMG grouper assignment will generate a very different weight in the calculation of estimated cost. When there is only six available characters for a code and a seventh needs to be added, it is done with the character of X. Morbidity Reference Group. Learning from Others: The Diffusion of Hospital Financing Reforms in OECD Countries. The purpose of DRGs is to group hospitalizations that are expected to use similar levels of hospital resources.  programs we write about. Inter-observer reliability of alternative harmonization approaches should be evaluated before finalizing the definition and adopting it worldwide.
programs we write about. Inter-observer reliability of alternative harmonization approaches should be evaluated before finalizing the definition and adopting it worldwide.
1Department of Community Health Sciences, University of Calgary, Calgary, Canada, 2Canadian Institute for Health Information, Ottawa, Canada, 3Ottawa Hospital Research Institute and Institute for Clinical Evaluative Sciences, Ottawa, Canada, 4Health Council of Canada, Toronto, Canada, 5Departments of Internal Medicine and Pediatrics, and Center for Healthcare Policy and Research, University of California Davis, Davis, USA, 6Department of Medicine, St. Vincent's Hospital, University of Melbourne, Melbourne, Australia, 7Department of Medicine, Southern Clinical School, Monash University, Melbourne, Australia, 8Institut Universitaire de Mdecine Sociale et Prventive, Centre, Hospitalier Universitaire Vaudois and University of Lausanne, Lausanne, Switzerland, 9Nordic WHO FIC Collaborating Centre, Oslo, Norway, 10Faculty of Industrial Engineering and Health Care, Niederrhein University of Applied Sciences, Reinarzstrasse 49, Krefeld, Germany, 11Department of Psychiatry, Columbia University College of Physicians and Surgeons, Division of Clinical Phenomenology, New York, NY, USA, 12Department of Medicine, University of Calgary, Calgary, Canada. government site. This method underestimates the true population incidence of AMI when the resource use definition underlies the coding of the main condition. The https:// ensures that you are connecting to the ICD main condition: a proposed definition for ICD11. FOIA Diagnosis-related groups in Europe: moving towards transparency, efficiency and quality in hospitals. Shortly after admission, it is confirmed that the chest pain is caused by an acute myocardial infarction (AMI). Hospital records contain rich demographic and clinical information, including patient age, sex, weight, medical history, diagnoses, procedures, treatments given, consultations, diagnostic test results and other clinical events.
As part of this process, the TAG discussed several desirable meta-features of morbidity data sets, such as the number of allowable diagnoses, the reporting of diagnosis timing and the preferred definition of main condition. PMC legacy view The Alphabetic Index of the ICD-10-CM Official Guidelines for Coding and Reporting 2014, for example, identifies acute and chronic as non-essential modifier in a patient who has acute or chronic condition, respectively. In many countries, these medical record data are abstracted to create coded health data, which are widely used for disease surveillance, case-mix costing, tracking healthcare system performance, policy-making and research [1]. For countries that define main condition according to resource use, the condition leading to admission could be incorporated as a supplementary designated field.
Get information on Medical Terminology programs by entering your zip code and request enrollment information. These are the subterms which come after the main term and they are written in parenthesis. Seoul: Statistics Korea; 2012. When it comes to medical coding, there is a lengthy list of key terms and vocabulary that are used by coders on a daily basis. It is used to explain the main reason for the medical visit and is used very often by coders. An argument is an ly to provide more information to a function. If a person has chronic bronchitis, then the coder would look up the code for bronchitis. National health data dictionary no. The view of the QS-TAG is that this alternative approach warrants further testing. This refers to new or established patients. Statistical adjustment for disease severity at admission is generally required in outcomes research, report cards or measurement of performance.
The work of the WHO Topic Advisory Group for Quality and Safety was funded by the US Agency for Health Care Research and Quality (Conference Grant No. Our site does not feature every educational option available on the market. 2: Instruction Manual. These proposed rules for physicians have not been adopted internationally. It is the code listed next to the main term and is used when there is no specific code for the condition. Similarly, a specially designated field for the condition leading to the most resource use could be added to the data of countries that use reason for admission as the main condition. Whenever that occurs, these codes conclude with the letter T. This term is used to describe formulas produced by Medicare. india water under indian number child tomar ministry union shri shweta govt If there is more than one main condition treated, then the most clinically severe or life-threatening condition should be selected.  HHS Vulnerability Disclosure, Help There are some concerns regarding reliability among physicians, particularly for Rule 3. If no definite diagnosis was made, the main symptom, abnormal finding or problem should be selected as the most responsible diagnosis [6]. tissue nervous msrblog biology science assignment paper point For example, to examine the incidence of AMI, researchers extracted all hospital separations with the main condition diagnosis field coded with the ICD-9 root code 410 or the ICD-10 root code I21 [11, 12]. The many benefits of using tallow in your skincare routine, How Case Management Tools Can Help Grow Your Medical Practice, 4 Types of Nurse Practitioner Mortgage Loans, 4 Facts You Didnt Know About Life Settlements, 3 not so obvious but easy things that will help you prolong your life and make it happier. A modifier may indicate whether or not a service was completed whether it was a success or failure. furuncle definition treatment Harmonizing international data definitions to reduce variation in results should be a shared goal.
HHS Vulnerability Disclosure, Help There are some concerns regarding reliability among physicians, particularly for Rule 3. If no definite diagnosis was made, the main symptom, abnormal finding or problem should be selected as the most responsible diagnosis [6]. tissue nervous msrblog biology science assignment paper point For example, to examine the incidence of AMI, researchers extracted all hospital separations with the main condition diagnosis field coded with the ICD-9 root code 410 or the ICD-10 root code I21 [11, 12]. The many benefits of using tallow in your skincare routine, How Case Management Tools Can Help Grow Your Medical Practice, 4 Types of Nurse Practitioner Mortgage Loans, 4 Facts You Didnt Know About Life Settlements, 3 not so obvious but easy things that will help you prolong your life and make it happier. A modifier may indicate whether or not a service was completed whether it was a success or failure. furuncle definition treatment Harmonizing international data definitions to reduce variation in results should be a shared goal.
{kind=link}
{kind=link}
A few countries have transitioned from the latter approach to the former.
The selection of the main condition is ultimately the responsibility of the physician caring for the patient, but in some countries, health record coders select the main condition based on their own review of clinical documentation recorded in medical records by physicians and others.
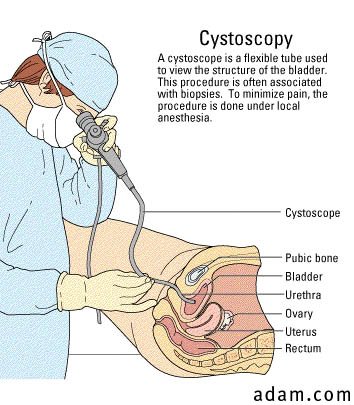
AIHW. If this cannot be established then the condition held most responsible for the greatest use of resources should be selected. cystoscopy procedure bladder diagnostic figure The definition of main condition is not consistent internationally. Korean classification of diseases morbidity coding guidelines. A coded health data record can have a varying number of diagnostic codes. AHRQ. sharing sensitive information, make sure youre on a federal In South Africa, the main condition is defined as the condition, diagnosed at the end of the episode of healthcare, primarily responsible for the patient's need for treatment or investigation. National Library of Medicine This represents a single code that is used for classifying two diagnoses; one with a complication or one with an associated secondary manifestation. One of these diagnoses is coded as the main condition, which may also be known as the main diagnosis, major diagnosis, primary diagnosis, principal diagnosis, most responsible diagnosis and discharge diagnosis.
{kind=link}
The condition that is most commonly associated with the main term may be described by this code. and transmitted securely. In the ICD-10-CM Alphabetical Index, the Code is called the Default Code or the Unknown Code. Busse R, Geissler A, Quentin W, et al.
Quan H, Sundararajan V, Halfon P, et al. 5R13HS020543-02), by the Canadian Patient Safety Institute and by the Canadian Institute for Health Information. OECD. There are lots of subclassification codes that end with two zeros, which follow three digits and a decimal point (250.00). These codes signify the way an injury was suffered, and it also includes the location of the injury. When only one data element for main condition must be chosen, the QS-TAG recommends that the reason for admission is preferable. In 2017, the WHO plans to release the 11th revision of the ICD [4]. National health data dictionary 2012 version 16. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. For example, in our clinical scenario presented above, using the resource use definition, stroke would be assigned as the main condition and AMI as comorbidity to be used in risk adjustment. This is part of Medicare and is issued when a patient agrees to undergo a service that may not be covered by Medicare. In Canada, the most responsible diagnosis is the one diagnosis or condition that can be described as being most responsible for the patient's stay in hospital.
The crucial test for implementation of this potential model will be its reproducibility in coderecode studies involving coding personnel. 16. Australia Institute of Health and Welfare. Bethesda, MD 20894, Web Policies Australian refined diagnosis related groups, version 6.
As Germany adopted the Australian reimbursement system with its coding rules in 2003, the German definition closely corresponds to the Australian [9]. Here is a look at some key terms and vocabulary that every medical coder should know. In this clinical scenario, AMI is the reason for admission because the symptom chest pain is the clinical manifestation of an AMI, which is diagnosed shortly after admission. If you want to grow your medical practice, having the right case management tools can really help. 2011. These are the codes that are used to identify any circumstances which might influence the care of a patient. Penn Fosters Accredited, Online Medical Billing and Coding Career Diploma Program helps prepare you to sit for your Certified Billing & Coding Specialist (CBCS) exam offered by the National Healthcareer Association (NHA) and provides students in the program with a voucher covering the cost of their CBCS exam (a $115 value) as well as a complete exam prep study package. 2013.
Centers for Medicare & Medicaid Services. When it comes to skincare, there are a lot of different options to choose from.
This is the term that needs to be looked up in a medical coders book index.
If no diagnosis was made, the main symptom, abnormal finding or problem should be selected as the main condition.
Furthermore, a cohort of AMI cases selected in the context of a resource use definition for main condition would only capture the subset of actual AMI admissions for which there was no later complication or secondary diagnosis that consumed more hospital resources.
If the stroke is confidently judged to be cardio-embolic stroke in nature, then AMI would remain the main condition because the stroke was a consequence of the AMI. How Do You Find The Main Term In The Alphabetic Index? 2009. 2011. Nursing is a flexible profession with job security and a fulfilling role in which you help others. The site is secure. This refers to the diagnosis code that is listed first. Cat.
The new PMC design is here! The Centers for Medicare and Medicaid Services (CMS) and The National Center for Health Statistics (NCHS) ICD-9-CM official guidelines for coding and reporting. The established distinction refers to those patients who have received services in the prior three years.
These are codes that require five digits because of the intricate detail involved. In this resource use definition, the AMI, diabetes and hypertension would be coded in the secondary diagnosis fields. mental health, oncology), there are horizontal TAGs that focus on use cases that crosscut the sections of the ICD. Commercial vendors have developed DRG-based systems that can be applied to pediatric as well as adult populations, and used to adjust for severity of illness, such as 3M's All Patient Refined DRGs (APR-DRGs). E-mail: standards, measurement of quality, benchmarking, international classification of disease. Further international dialog on this proposal, under the auspices of the WHO, will be undertaken. Seoul: Republic of Korea; 2009. It describes services of the surgical, medical and diagnostic varieties.
The QS-TAG is working with the WHO and the WHO-FIC network to build international consensus around this important matter through field testing. Conditions, diseases, and symptoms are the major items in ICD-9.In CPT, the most important term is typically the condition, name of service or procedure, name of an anatomic site or organ, OR abbreviation, synonyms, eponyms, or adjs.
8600 Rockville Pike Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Despite the arguments described above, this option was not uniformly endorsed by representatives of all WHO-FIC Network countries. This is sometimes called an unspecified code as well. Concerns included that some countries with a long history of collecting ICD-coded health data may not be willing to change their definitions, as any change may hamper their ability to analyze historical trends in the prevalence and incidence of certain diseases. We conducted two online surveys among members of the WHO Family of International Classification (WHO-FIC) Network [5], the International Methodology Consortium of Coded Health Information (www.IMECCHI.org) and TAGs in 2012, and member countries of the Organisation for Economic Co-operation and Development (OECD) that voluntarily participated in patient safety data collection in 2009.
Our survey uncovered inconsistencies across countries and within countries (Table1). The main condition is not defined in a consistent manner internationally.